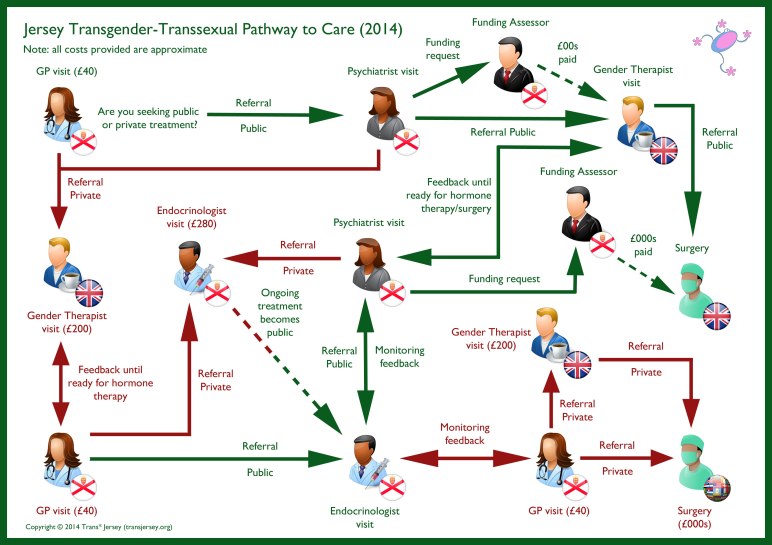
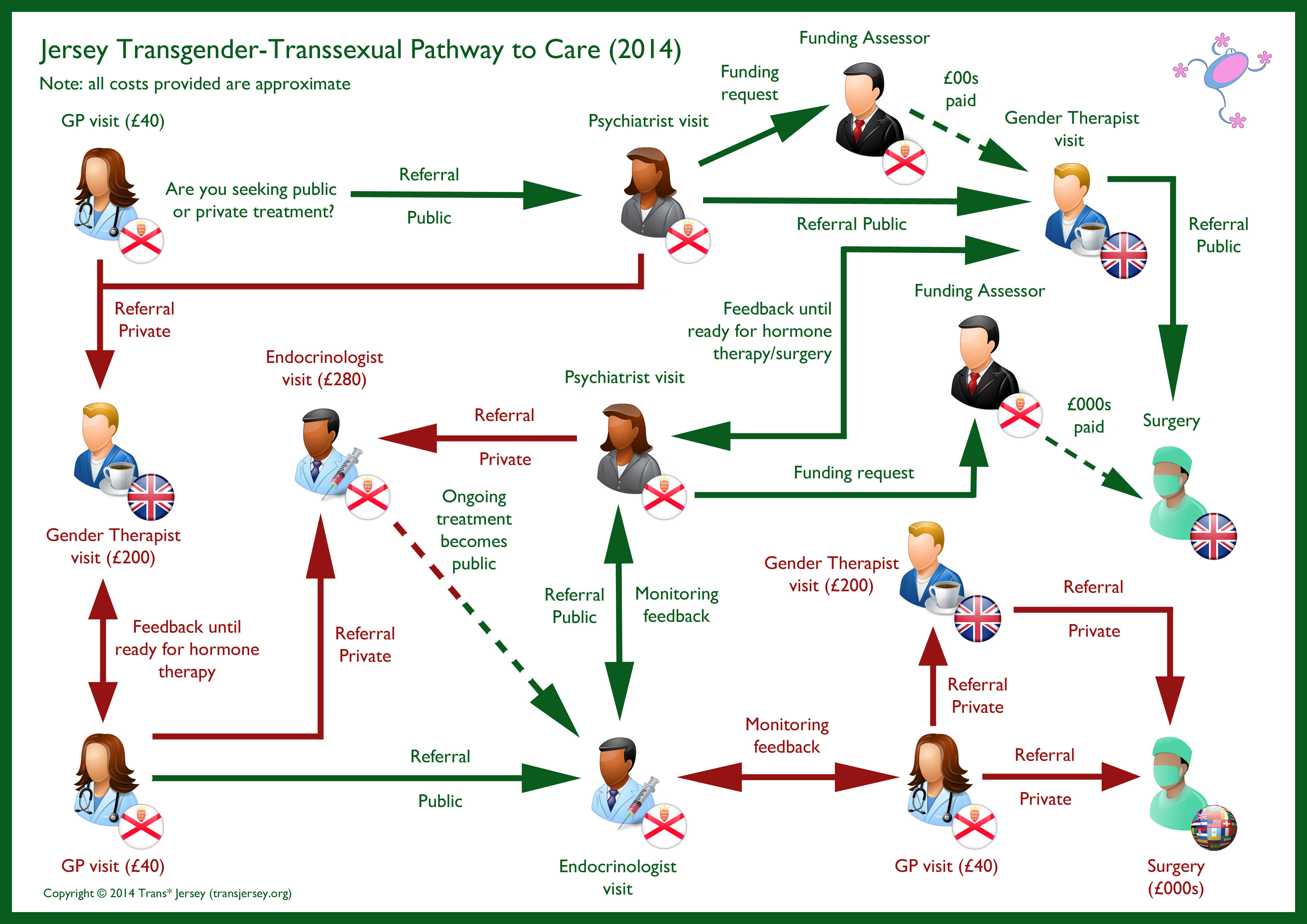
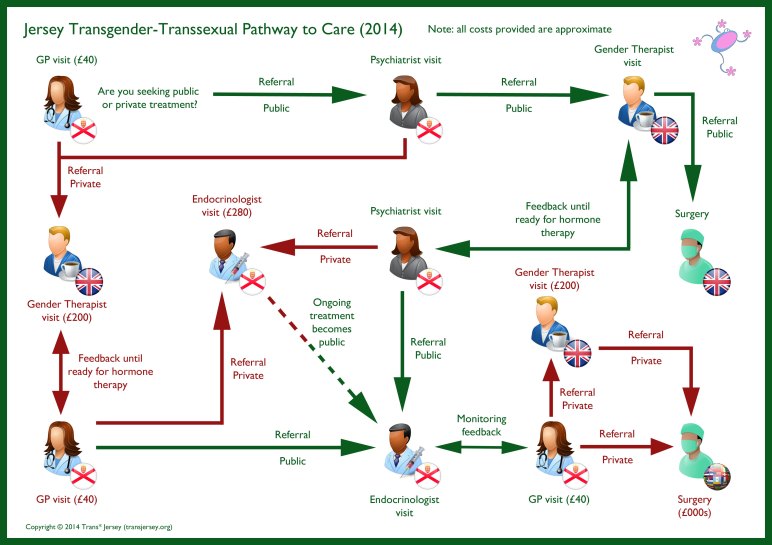
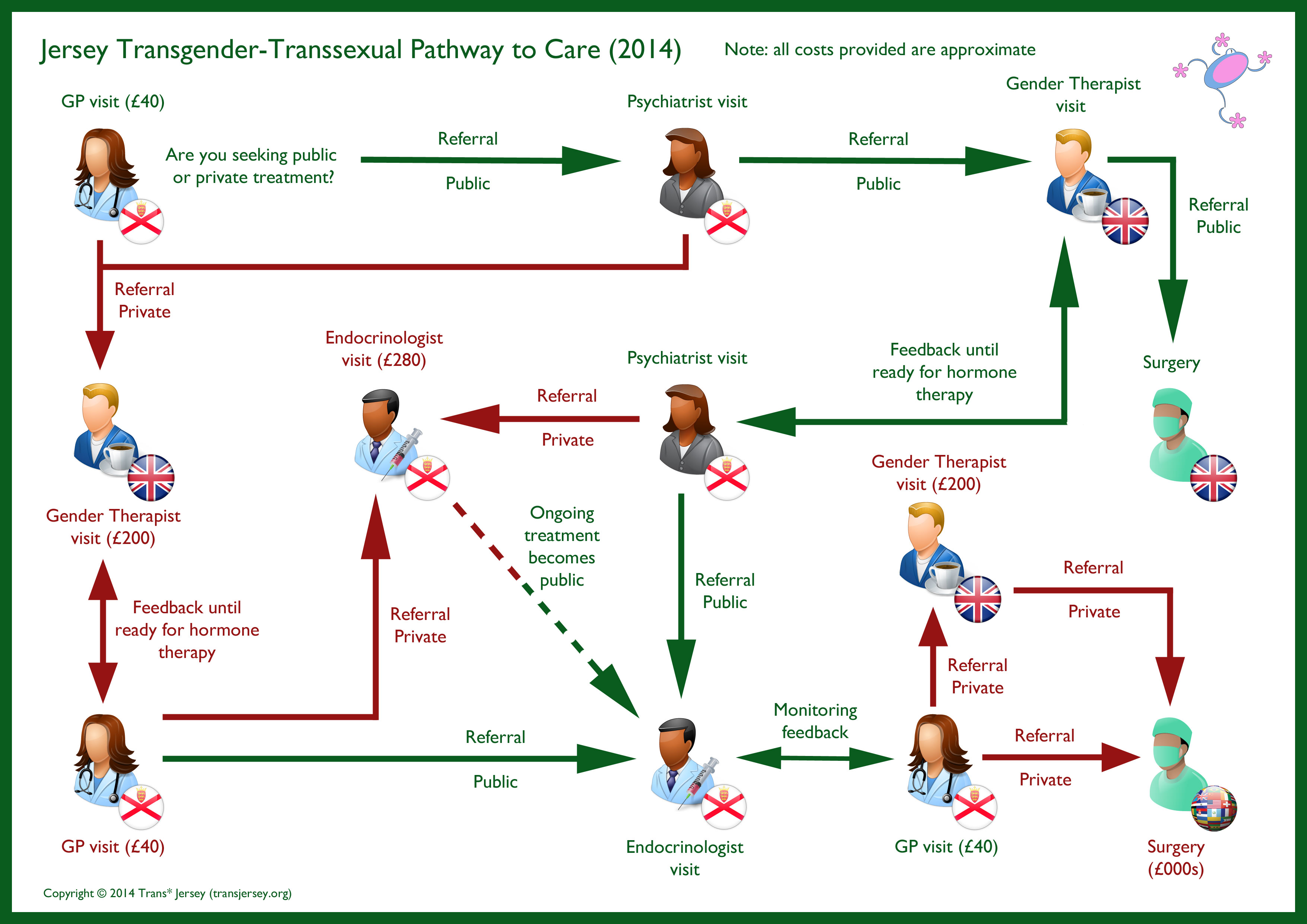
Because there are no specialist gender healthcare professionals in Jersey, all trans* islanders have to go abroad for treatment. Most will, at least initially, go to the UK. Therefore, any issues that trans* organisations have with the UK healthcare system are shared by Jersey trans* individuals.
In addition to producing a report on the health of trans* individuals, GIRES also identifies three main areas of concern:
Multiple referral for treatment
Current treatment protocols often require two referrals before cross sex hormones, or chest reconstruction, or genital surgery, etc are authorised. This causes delays. No other medical treatment requires two referrals so why are trans people singled out for a “special” treatment protocol.
 Refusal to treat
Refusal to treat
If a trans person has been treated for gender dysphoria in the private system or overseas, that person’s treatment on the NHS may be delayed. No other such patient is refused treatment on the NHS for any other condition.
Health providers must be challenged to provide the equality analysis that justifies treating trans people in a different manner from other service users.
Delays in receiving treatment for young people
A young trans person can benefit hugely from an early medical intervention to ensure that the damage done, both physically and psychologically, from an inappropriate puberty can be minimised, where there is a clear clinical need established.
Delaying treatment for young people can have a disproportionate impact. A delay of (for example) three years in treating a 30 year old gender dysphoric person will not significantly change the physical outcome on the transition as the individual will have already developed adult sexual characteristics. However, for the 11 year old, the situation is completely different. However, both patients will suffer psychological stress due to the delay.
Again, Health providers must be challenged to provide the equality analysis that justifies treating trans people in a different manner from other service users.
As we have stated elsewhere, it should be noted that Jersey trans* people can avoid some or all of the above problems if they have the resources to navigate the system privately or semi-privately. In which case, they may not find the above to be an issue in their transition.